Meeti ng evacuees’ emergency medical needs
while maintaining Dallas’ EMS operati onal capabiliti es
S. Marshal Isaacs, MD, FACEP, FAEMS
Professor of Emergency Medicine/Department of Emergency Medicine, UT Southwestern Medical Center
Medical Director, UTSW/BioTel EMS System, Dallas Fire-Rescue Department
W
Att ending emergency physician at Parkland Memorial Hospital hen I came to
Dallas in 2005,
it was just after
Dallas had stood up
for a major sheltering
medical operation for
evacuees from Hurricane Katrina. Over the
past decade, during which I’ve served as the
medical director for Dallas Fire-Rescue, I
have heard nothing but praise for the eff orts
of the many individuals and organizations
who contributed to that eff ort. Th erefore,
when Hurricane Harvey made landfall in
South Texas and the scope of the devastation
began to emerge, I wanted to help in any way
possible to make Dallas’ response as good as,
if not better than, it was after Katrina.
My role with Dallas Fire-Rescue includes
assisting Dallas Fire Chief David Coatney
and his command staff to ensure that
Dallas fi refi ghters and paramedics who
provide emergency medical coverage to any
special event or mass gathering in Dallas
have the appropriate education, training,
policies, protocols, and equipment to do the
exemplary work they do each day. Th us, early
on Aug. 28, at the direction of the fi re chief
and DFR Assistant Chief Daniel Salazar, the
EMS Bureau’s command staff convened at
DFR EMS headquarters to begin planning
the emergency medical services support of
the proposed “Megashelter” at the Kay Bailey
Hutchison Convention Center.
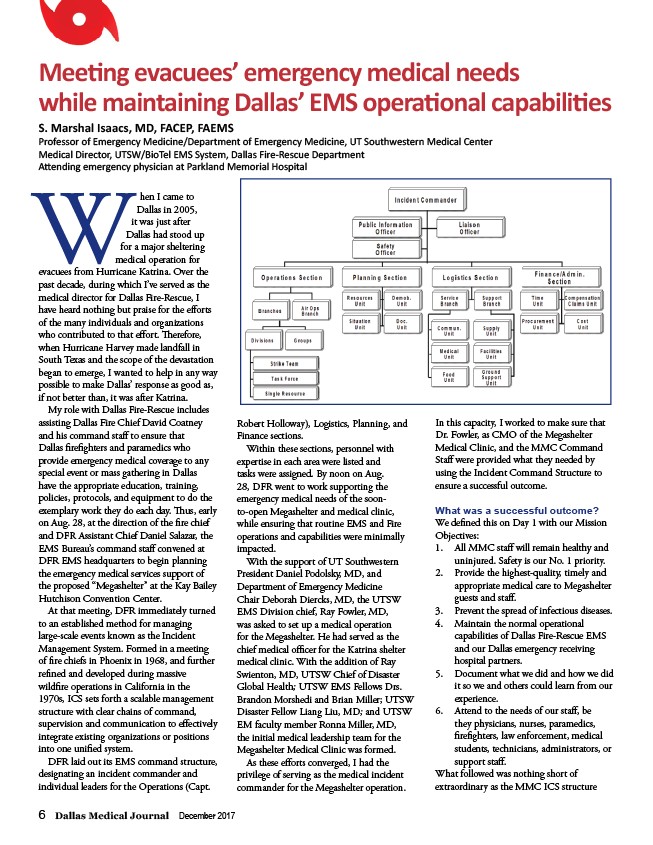
At that meeting, DFR immediately turned
to an established method for managing
large-scale events known as the Incident
Management System. Formed in a meeting
of fi re chiefs in Phoenix in 1968, and further
refi ned and developed during massive
wildfi re operations in California in the
1970s, ICS sets forth a scalable management
structure with clear chains of command,
supervision and communication to eff ectively
integrate existing organizations or positions
into one unifi ed system.
DFR laid out its EMS command structure,
designating an incident commander and
individual leaders for the Operations (Capt.
6 Dallas Medical Journal December 2017
Robert Holloway), Logistics, Planning, and
Finance sections.
Within these sections, personnel with
expertise in each area were listed and
tasks were assigned. By noon on Aug.
28, DFR went to work supporting the
emergency medical needs of the soonto
open Megashelter and medical clinic,
while ensuring that routine EMS and Fire
operations and capabilities were minimally
impacted.
With the support of UT Southwestern
President Daniel Podolsky, MD, and
Department of Emergency Medicine
Chair Deborah Diercks, MD, the UTSW
EMS Division chief, Ray Fowler, MD,
was asked to set up a medical operation
for the Megashelter. He had served as the
chief medical offi cer for the Katrina shelter
medical clinic. With the addition of Ray
Swienton, MD, UTSW Chief of Disaster
Global Health; UTSW EMS Fellows Drs.
Brandon Morshedi and Brian Miller; UTSW
Disaster Fellow Liang Liu, MD; and UTSW
EM faculty member Ronna Miller, MD,
the initial medical leadership team for the
Megashelter Medical Clinic was formed.
As these eff orts converged, I had the
privilege of serving as the medical incident
commander for the Megashelter operation.
In this capacity, I worked to make sure that
Dr. Fowler, as CMO of the Megashelter
Medical Clinic, and the MMC Command
Staff were provided what they needed by
using the Incident Command Structure to
ensure a successful outcome.
What was a successful outcome?
We defi ned this on Day 1 with our Mission
Objectives:
1. All MMC staff will remain healthy and
uninjured. Safety is our No. 1 priority.
2. Provide the highest-quality, timely and
appropriate medical care to Megashelter
guests and staff .
3. Prevent the spread of infectious diseases.
4. Maintain the normal operational
capabilities of Dallas Fire-Rescue EMS
and our Dallas emergency receiving
hospital partners.
5. Document what we did and how we did
it so we and others could learn from our
experience.
6. Attend to the needs of our staff , be
they physicians, nurses, paramedics,
fi refi ghters, law enforcement, medical
students, technicians, administrators, or
support staff .
What followed was nothing short of
extraordinary as the MMC ICS structure