Mass-scale sheltering of Hurricane Harvey evacuees:
Infectious disease surveillance and prevention
Wendy Chung, MD
Dallas County Health and Human Services, Chief Epidemiologist
A s Hurricane Harvey made landfall
Figure 1. near Rockport as a Category
4 hurricane on Aug. 25, two
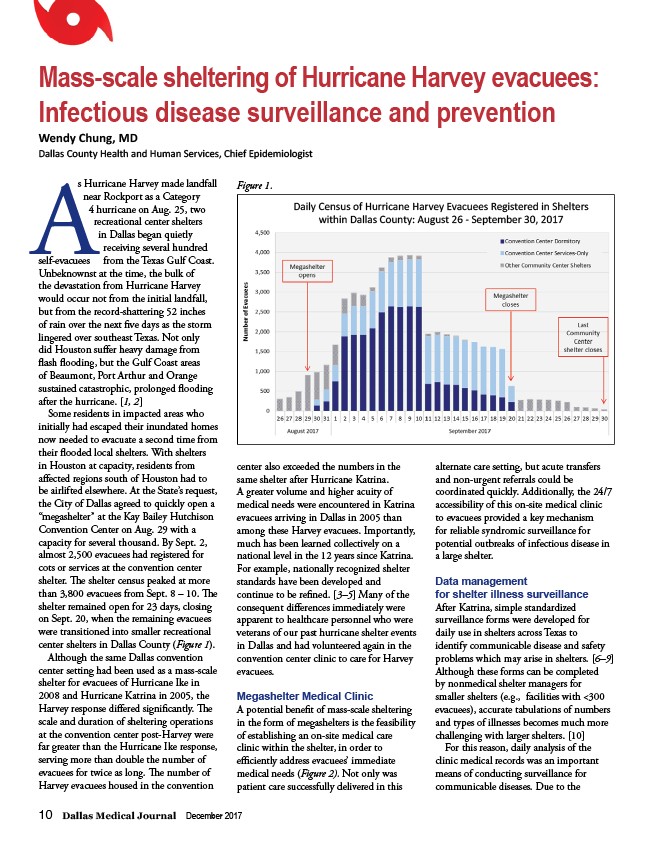
Daily Census of Hurricane Harvey Evacuees Registered in Shelters
recreational center shelters
in Dallas began quietly
receiving several hundred
self-evacuees from the Texas Gulf Coast.
Unbeknownst at the time, the bulk of
the devastation from Hurricane Harvey
would occur not from the initial landfall,
but from the record-shattering 52 inches
of rain over the next fi ve days as the storm
lingered over southeast Texas. Not only
did Houston suff er heavy damage from
fl ash fl ooding, but the Gulf Coast areas
of Beaumont, Port Arthur and Orange
sustained catastrophic, prolonged fl ooding
after the hurricane. 1, 2
Some residents in impacted areas who
initially had escaped their inundated homes
now needed to evacuate a second time from
their fl ooded local shelters. With shelters
in Houston at capacity, residents from
aff ected regions south of Houston had to
be airlifted elsewhere. At the State’s request,
the City of Dallas agreed to quickly open a
“megashelter” at the Kay Bailey Hutchison
Convention Center on Aug. 29 with a
capacity for several thousand. By Sept. 2,
almost 2,500 evacuees had registered for
cots or services at the convention center
shelter. Th e shelter census peaked at more
than 3,800 evacuees from Sept. 8 – 10. Th e
shelter remained open for 23 days, closing
on Sept. 20, when the remaining evacuees
were transitioned into smaller recreational
center shelters in Dallas County (Figure 1).
Although the same Dallas convention
center setting had been used as a mass-scale
shelter for evacuees of Hurricane Ike in
2008 and Hurricane Katrina in 2005, the
Harvey response diff ered signifi cantly. Th e
scale and duration of sheltering operations
at the convention center post-Harvey were
far greater than the Hurricane Ike response,
serving more than double the number of
evacuees for twice as long. Th e number of
Harvey evacuees housed in the convention
within Dallas County: August 26 - September 30, 2017
center also exceeded the numbers in the
same shelter after Hurricane Katrina.
A greater volume and higher acuity of
medical needs were encountered in Katrina
evacuees arriving in Dallas in 2005 than
among these Harvey evacuees. Importantly,
much has been learned collectively on a
national level in the 12 years since Katrina.
For example, nationally recognized shelter
standards have been developed and
continue to be refi ned. 3–5 Many of the
consequent diff erences immediately were
apparent to healthcare personnel who were
veterans of our past hurricane shelter events
in Dallas and had volunteered again in the
convention center clinic to care for Harvey
evacuees.
Megashelter Medical Clinic
A potential benefi t of mass-scale sheltering
in the form of megashelters is the feasibility
of establishing an on-site medical care
clinic within the shelter, in order to
effi ciently address evacuees’ immediate
medical needs (Figure 2). Not only was
patient care successfully delivered in this
10 Dallas Medical Journal December 2017
alternate care setting, but acute transfers
and non-urgent referrals could be
coordinated quickly. Additionally, the 24/7
accessibility of this on-site medical clinic
to evacuees provided a key mechanism
for reliable syndromic surveillance for
potential outbreaks of infectious disease in
a large shelter.
Data management
for shelter illness surveillance
After Katrina, simple standardized
surveillance forms were developed for
daily use in shelters across Texas to
identify communicable disease and safety
problems which may arise in shelters. 6–9
Although these forms can be completed
by nonmedical shelter managers for
smaller shelters (e.g., facilities with <300
evacuees), accurate tabulations of numbers
and types of illnesses becomes much more
challenging with larger shelters. 10
For this reason, daily analysis of the
clinic medical records was an important
means of conducting surveillance for
communicable diseases. Due to the